
Content advisory: chock full of anatomical terms, some reproductive processes talk.
Welcome to the QueerDoc Gettin’ Square blog series! We’ll be talking about all things testosterone over the next couple of weeks and some non-testosterone ways to present in squarer, more angular ways. This week, we get nerdy about sex steroid hormones (heavy on the testosterone) and how they are generated and maintained in the body. Next week we’ll talk about what forms of testosterone are used in gender affirming care, some of the risks and benefits of testosterone, and a timeline of what changes are expected and when.
Phew! The human endocrine system is mighty complex, and we’re constantly learning more. Today, we’ll go over some of the main bits.
As we mentioned last week, hormones are messengers – they travel to and tell other parts of the body to do things. Hormones in the body are created and regulated by the endocrine system. The endocrine system is comprised of glands that, when prompted, create or release hormones. These hormones travel through the body to a target cell and tell the target cell to do something.
Endocrine glands secrete hormones into the space immediately surrounding them. From there, the hormones may work directly on the cells in that area or enter the bloodstream for dispersal throughout the body.
There are also two main types of hormones: water-soluble and lipid (fat)-soluble. Water-soluble hormones travel freely in the bloodstream. Lipid-soluble hormones must hitch a ride on a protein to circulate in the bloodstream. Sex steroid hormones–testosterone, estrogen, and progestin (and their derivatives)– are fat-soluble. Nerd tip: your body needs cholesterol to produce hormones!
Hormones must be able to attach to the target cell to deliver their messages. They do this via receptors. This is how (most) hormones work on some cells and not others. Once at a cell and matched to a receptor, hormones can do various things. They may change the cell membrane so that other chemicals or signals can travel more or less easily. The hormone can tell the cell to turn on/off or up/down other processes within the cell or tell the cell to secrete different hormones. Lipid-soluble hormones can enter the cell and may attach directly to DNA.
Hormones also interact with each other and may bind to each other. When they do this, they might increase or decrease the ability of their partner hormone to be recognized and used by their target cells.
The glands that are important to sex steroid hormone production are:
- The hypothalamus
- The pituitary
- The ovaries or testes
- The adrenal glands
Other tissues in the body also produce hormones, but that’s a talk for another day!
The main hormones we’re going to talk about today are:
- Gonadotropin-releasing hormone (GnRH)
- Follicle-stimulating hormone (FSH)
- Luteinizing hormone (LH)
- Androgens
- Testosterone
- DHEA
- DHT
- Estrogens
- Estradiol (this is what we prescribe in gender affirming care for gettin’ curvy)
- Estrone (a weak estrogen that can convert to estradiol)
- Estriol (produced during pregnancy, may have immune-supportive effects)
- Progesterone
- Proto-hormones
- Androstenedione
And an enzyme or two: Aromatase and 5-alpha Reductase.
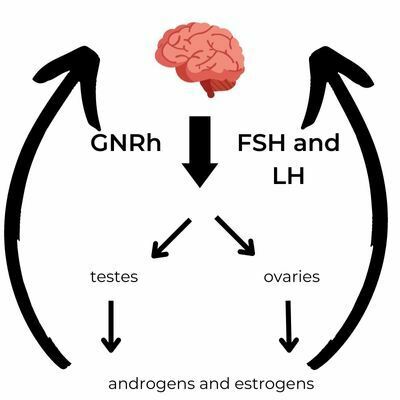
It’s all a feedback loop: the hypothalamic-pituitary-gonadal axis.
The hypothalamus is deep in the brain behind your sinus cavities and at the top of the brain stem. One of its functions is to create gonadotropin-releasing hormone (GnRH.)
GnRH enters the bloodstream and goes forth to find its target receptors in the pituitary gland, conveniently right next door. GnRH tells the pituitary to make follicle-stimulating hormone (FSH) or luteinizing hormone (LH.)


Nerd tip: the pituitary interprets which hormone to make according to the frequency of GnRH pulses from the hypothalamus.
FSH and LH then travel to their target cells. In people with ovaries, the target cells are in and around the follicles in the ovary, which hold developing eggs. LH binds to cells surrounding the follicle and prompts aromatase and androgen production (we’ll circle back to aromatase later.) FSH binds to follicle cells and tells the cells to use the androgens nearby to create estrogens. Estrogen production ramps up during the maturation of a gamete, then drops after ovulation. At ovulation, another structure, the corpus luteum, is formed, and the corpus luteum secretes a message to the hypothalamus that tells it to calm down. The corpus luteum also creates progesterone.
The hypothalamus senses the levels of androgens and estrogens in the bloodstream (and the message from the corpus luteum) and releases more or less GnRH in response. When blood levels of estrogens are high, the hypothalamus secretes less GnRH. When blood levels of estrogens are low, the hypothalamus secretes more GnRH.
And around and around it goes.
Other tissues in the body also create and secrete hormones, including the adrenal glands. Adrenal glands are located just on top of the kidneys, and they produce DHEA and androstenedione (and other essential hormones like cortisol and adrenaline.)
DHEA (Dehydroepiandrosterone)

DHEA is both a building block for estrogens and testosterone and a hormone in its own right: it also attaches to receptors in target cells and tells them to do things.
DHEA can bind to estrogen and testosterone receptors and act as them. It also converts to testosterone and DHT(dihydrotestosterone) in the skin and hair follicles: DHEA is what triggers armpit and pubic hair growth in early puberty, increases skin oil and sweat production, and causes stinky adult sweat. (More on DHEA and hair in two weeks!)
Androstenedione

Androstenedione is produced by gonads (ovaries and testes) and the adrenal glands and can be converted to either testosterone or estrone. Post-menopause, androstenedione is the primary hormone produced by ovaries.
There are so many ests and tests!
And, there are more than we’re talking about today! Many of them play intermediate roles in the production of other hormones.
But, we’re Gettin’ Square, Right?
What does this mean when you’re adding testosterone to bodies with ovaries?
The hypothalamus also responds to levels of testosterone in the blood. When testosterone levels are high, the hypothalamus decreases the production of GnRH. Less GnRH reaches the pituitary gland, so less FSH and LH are released, and the ovaries are not prompted to start their hormone production of androgens and estrogens.
Testosterone in gender affirming care is all about moderation.
Why?
Androgens can convert to estrogens.
In fact, all estrogens in the body are created by conversion from androgens.
The enzyme aromatase is the key to these conversions (we mentioned aromatase back when discussing what LH and FSH do!)
Aromatase is found in multiple places in the body: in ovaries and testicles, in fat cells, blood vessels, bone cells, skin cells, placental cells, in the brain and in bone. However, in people with ovaries, it is produced by the ovaries. Age, increased fat stores, insulin, alcohol, and our friends FSH and LH all increase aromatase activity.
It would be logical to conclude that:
- When testosterone is added to the body, the hypothalamus notices and lowers FSH and LH production
- The ovaries, receiving less FSH and LH, reduce aromatase production
- With less aromatase, fewer estrogens are produced.
But this isn’t quite how it works.
In the absence of FSH, testosterone triggers aromatase production.
This is why a higher dose of testosterone in gender affirming care is not advised: we don’t want to add so much testosterone to the body that it converts to estrogens.
There are some tools to prevent aromatase production, and thus estrogen production: aromatase inhibitors (anastrozole, letrozole, and exemestane.) These medications commonly treat hormone-dependent cancers such as breast, uterine, and prostate cancers. They are less frequently used to treat endometriosis, stimulate ovulation, and disorders of sex hormone production. They are not commonly used in gender affirming care due to side effects. At QueerDoc, we may occasionally use anastrozole to stop menstruation, but we don’t like doing so for long periods of time.
5-alpha Reductase
5-alpha reductase is present in muscle tissue and converts testosterone to DHT.
Testosterone and DHT use the same receptors, but DHT binds more efficiently than testosterone.
Too much DHT is a factor in:
- Hair loss at the crown of the head
- Excess facial and body hair in people with ovaries
For people who have ovaries, are taking testosterone, and are concerned about balding, drugs that inhibit 5-alpha reductase (finasteride, dutasteride) can limit scalp hair loss by lowering the amount of 5-alpha reductase available to convert testosterone to DHT. We’ll discuss DHT more in 2 weeks when we talk about hair and contraception!.
For super nerdy fun, here are the conversions:

Please let us know what else you’d like to learn about testosterone in the body!
References
- Sheng JA, Tan SML, Hale TM, Handa RJ. Androgens and Their Role in Regulating Sex Differences in the Hypothalamic/Pituitary/Adrenal Axis Stress Response and Stress-Related Behaviors. Androg Clin Res Ther. 2021 Dec 23;2(1):261-274. doi: 10.1089/andro.2021.0021. PMID: 35024695; PMCID: PMC8744007.
- Stocco C. Tissue physiology and pathology of aromatase. Steroids. 2012 Jan;77(1-2):27-35. doi: 10.1016/j.steroids.2011.10.013. Epub 2011 Nov 13. PMID: 22108547; PMCID: PMC3286233.
- Ali, Emad S. MD1; Mangold, Cheyenne MSIII2; Peiris, Alan N. MD, PhD, FRCP(London)3 Estriol: emerging clinical benefits, Menopause: September 2017 – Volume 24 – Issue 9 – p 1081-1085 doi: 10.1097/GME.0000000000000855
- https://www.hopkinsmedicine.org/health/conditions-and-diseases/adrenal-glands#:~:text=Adrenal%20glands%2C%20also%20known%20as,stress%20and%20other%20essential%20functions.
- https://www.verywellhealth.com/what-is-dihydrotestosterone-4684657
- https://en.wikipedia.org/wiki/Aromatase
- https://www.ncbi.nlm.nih.gov/books/NBK557856/
- https://www.sciencedirect.com/science/article/abs/pii/S0306453018312307?via%3Dihub
- https://en.wikipedia.org/wiki/Dehydroepiandrosterone