This blog starts our Surgery Series. For the next few months, we will write about a different gender affirming surgery or procedure each week. This blog will discuss general preparation, timelines, and important things to know when getting ready for bottom surgeries. Content advisory: we’ll use anatomical terminology throughout this blog and the series.
THE WHAT
“Bottom surgeries” are a group of procedures used to more closely align an individual’s genitals to their gender. At QueerDoc, we believe there is NO ONE WAY to be trans and many ways to change your body. We are thrilled that surgeons are continuing to develop new techniques for gender affirming surgeries, and more options are available to individuals.
Many terms have been used for “bottom surgery,” some of which are now considered dated or offensive. You may see the acronyms “SRS,” “GRS,” or “GAS.” All these refer to surgery that changes the appearance, presence, and/or function of the genitals or reproductive organs. Most people and surgeons categorize surgeries as “feminizing,” “masculinizing,” or “non-binary.” We like to describe procedures by WHAT THEY DO rather than with an adjective, as “feminine,” “masculine,” and “non-binary” mean different things to different people.
When we refer to bottom surgeries, we mean
- Nulloplasty or Nullification
- Vaginectomy
- Penectomy
- Orchiectomy (with or without scrotomectomy)
- Phallus preserving vulvovaginoplasty
- Vaginal preserving phalloplasty
- Phalloplasty
- Metoidioplasty
- Vulvovaginoplasty
- Scrotoplasty
- Hysterectomy (with or without oophorectomy)
Get Your Greek and Latin On – Surgical Terms:
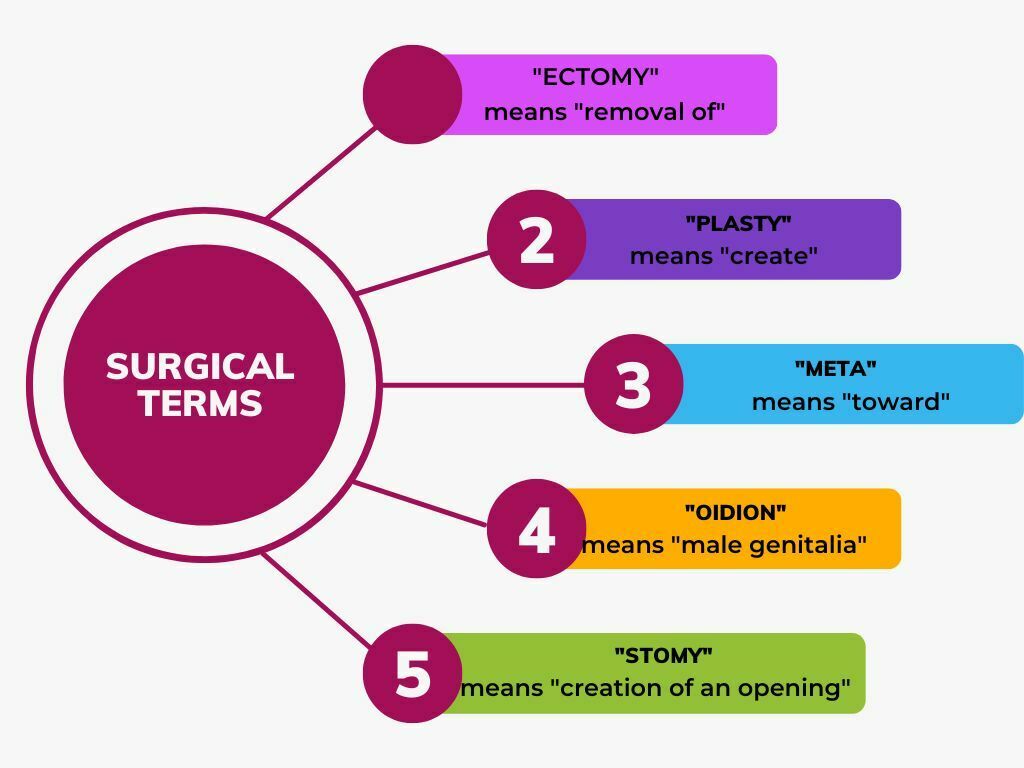
Therefore, a “vaginectomy” is the removal of the vagina while a “penectomy” is the removal of the penis, and “orchiectomy” is the removal of the testicles. “Phalloplasty” is the creation of a penis, while “vulvavaginoplasty” is the creation of a vulva and vagina. “Metoidoplasty” is the management of ligaments and tissues to allow the clitoris to move into a lower and more forward position, as a penis.
“Nulloplasty” is the removal of genitals. This surgery is fairly new, and creates a smooth pubic area with no genitals.
“Phallus preserving vulvavaginoplasty” and “vaginal preserving phalloplasty” keep the one and create the other.
We think it is super exciting that so many options are available.
THE WHEN
Expected prep and recovery will be somewhat different for each surgery, and we’ll go into detail in subsequent blogs. Here are some general tips:
Hair Removal
Many hair removal surgeries require hair removal before the operation. This is to:
- prevent hair from growing inside new structures, where it could cause dysphoria, irritation, or infection.
- Prevent the need for hair removal after surgery in or on structures that don’t normally have significant amounts of hair such as the inner labia, the vaginal canal, or the penile shaft.
IMPORTANT: you can start hair removal before your surgical consult. It may take up to 18 months to achieve sufficient hair removal, so starting early may be a good plan for you. Your surgeon will tell you their hair removal requirements. You can read more about hair removal for vaginoplasty at mtfsurgery.net and about hair removal for phalloplasty at phallo.net.
TIP: some insurance plans cover hair removal. Check your plan for details.



Physical Prep
Optimizing your health and nutrition before surgery can help you heal after surgery. Supporting your body with tools for healing can help you have a better overall experience.
If you are able to, consider consultations with professionals who can help you reach your goals, including:
- Nutrition experts
- Physical therapists
- Personal coaches
We contacted one of our favorite physical therapists, Brianna Durand, PT, DPT, of Empower Physiotherapy, who specializes in pelvic floor therapy for some thoughts about how a physical therapist can help you prepare for surgery (and get acquainted with your changed body after surgery!) Here’s what she had to say:
Pelvic floor physical therapy and bottom surgery- how (and when) do they coincide?
Well, if you’ve had a chance to read our other blogs about your pelvic floor, kegels, and reverse kegels, you’ve learned that there are a bunch of vital muscles in your pelvis. In the last decade or so, surgeons have finally begun embracing the role of pelvic floor PTs after bottom surgery, primarily vaginoplasty, and for a good reason. A growing amount of research shows that pelvic floor physical therapy helps improve symptoms such as pain, urinary leakage, difficulty achieving orgasm, and more. All of this is excellent news!
However, just like many other surgeries where muscles are cut and moved, waiting until after surgery isn’t always the best idea. Prehab–getting an evaluation and the indicated treatment before bottom surgery– will set you up best for success. Studies find that many patients have pelvic floor concerns before surgery. Addressing these concerns before surgery can help with healing and subsequent results. Think about it: if someone is already struggling with pain, urinary leakage, or other symptoms before bottom surgery, it’s pretty unlikely that underlying issues will be fixed by surgery.
All that to say, seeing a pelvic floor specialist can help you address any concerns you may have about various functions such as bowel/bladder, pain with sex, orgasm strength, prolapse, and even low back and hip pain. After bottom surgery, your primary focus is going to be on healing your tissue so you can start using your new anatomy! With pelvic floor PT beforehand, you can go into surgery as prepared as possible so that you have one less thing to worry about in the post-op phase. This isn’t to say that if you had your surgery years ago, it is too late to address any issues you’re experiencing now! If you’re experiencing any of the above symptoms, consider reaching out to a pelvic floor specialist near you.
Some surgeons have BMI limits and may require you to be under a certain BMI for surgery.
QUEERDOC NOTES:
We at QueerDoc support HAES (Health At Every Size.) A BMI requirement for surgery does not reflect our values, but we recognize that it exists*. If your surgeon has a BMI limit and this is a barrier for you, consider talking to your primary care provider, hormone provider, or surgeon about ways to help you reach your goals.
*some restrictions are due to the availability of medical equipment, such as tables and tools designed for larger bodies. We consider this a reflection of societal bias and believe that the industry should invest in tools that support medical care for all bodies.
Substance Use:
Alcohol and tobacco use can impair your healing ability, as can the use of illicit substances. We’re into harm reduction here, so we’re not interested in lecturing. However, what we really want to emphasize is cannabis and cocaine use.
Using cannabis or cocaine, when mixed with anesthesia, can be deadly.
Be very honest with your anesthesiologist if you use. It can save your life.
Hormones:
Will you need to stop hormones before surgery, and how long before surgery? Some surgeons no longer require that you stop your hormones, which may be a factor in choosing your surgeon.
Day of and Recovery:
Recovery is also slightly different for each surgery, and your surgeon should give you detailed information about what to expect and do. Here are some general things to consider:
- Where will you stay immediately after surgery and in the first few weeks?
- Who will drive you to/from surgery? (NOTE: Medicaid will pay for transportation.)
- Do you have a caretaker for the first few days/week?
- What will your physical limitations be and how will they change with time?
- Will you need certain kinds of clothing or equipment?
- How much time will you need to take off after work?
- What kinds of medical supplies will you need?
- Will you or a caretaker need to know how to change bandages or empty drains?
- What does healing look like?
- There are several reddits, facebook communities, and other websites dedicated to bottom surgery informatino and pictures at all stages from day one to years after.
- What should you do if
- You get nauseated or vomit
- Your stitches pop
- Your incisions get infected or you show signs of infection
- You have unexpected pain or bleeding
WHO:
How to Find and Choose A Surgeon
There are many surgeons in the United States and the world who offer bottom surgeries. Finding and choosing the right one for you can be an intricate process, and your choice may be narrowed due to insurance and financial restrictions. For each surgery, we’ll include links to surgeons known to us who offer that procedure.
We have a limited database of surgeons by procedure on our Gender Affirming Surgery page. It was designed for our internal use, so it contains medical terminology. Use with caution.
Some other directories of surgeons include
- TransHealthCare.org
- Phallo.net for phalloplasty
- findplasticsurgery.org
- WPATH Provider Directory
- OutCare Health
- mtfsurgery.net
- ftmsurgery.net
- The r/TransSurgeries wiki on Reddit
Factors that may help you choose your surgeon:
- Pictures of their previous surgeries
- Reviews from other patients
- Their rate of revisions and infections (and how they respond to unexpected results)
- Location
- If travelling, are there local housing options that are affirming
- Insurance plans they accept
- Their education and who they trained with
- Are they board certified?
- How much support they and their administrative staff can provide
- How much post-op support they provide
- Their willingness to work with you to achieve your desired looks and functions
- Are they willing to combine procedures on different parts of the body (could you get chest surgery and bottom surgery same day?)
- Do they have a BMI limit? An age limit?
- How long is their wait list
TIP: revisions are common. What is their revision policy?
HOW:
Common surgeon and insurance requirements
Surgeons and insurance often require:
- That you have been on hormones for a certain length of time
- WPATH SOC8 now recommends a minimum of six months
- You may be able to obtain surgery without any hormone use (this depends on the surgery, and may require prior authorization)
- Letters from your hormone provider/primary care provider
- Letters from mental health providers
- You can demonstrate the capacity to make an informed decision about your medical care
- Your surgeon will require a consult
Either may also require that:
- You have lived in a role congruent with your gender for a certain period of time
- Have documented support available after surgery
Often, your surgeon’s administrative staff will have people dedicated to helping you navigate insurance. If you run into barriers, consider working with a care navigator. We provide care navigation and love to refer people to TransFamily Support Services for free insurance navigation and support.
TIP: insurance may require that your letters are no more than one year old. If your surgery date is more than one year out or your surgery gets rescheduled, you may need to obtain a new set of letters.
Timeline TIP: some surgeries, particularly phalloplasty, happen in multiple stages, with a few months in between each surgery.
WHY:
Some things to think about when choosing which type of surgery you want
FORM and FUNCTION
What do you want your body to look like?
- Genitals are as individual as fingerprints. A good surgeon can help you understand what your new genitals may look like and what may or may not be possible for you.
- What is your surgeon’s ‘style’? Are they able and willing to create the form you want?
How do you want to use your genitals?
- Is orgasmic ability important to you?
- Is sexual activity important to you? If so, what kinds of sexual activity are you interested in?
What’s our schedule?
Subject to change, of course.
10/24 – Nulloplasty
10/31 – Vaginectomy
11/7 – Penectomy
11/14 – Orchiectomy with and without scrotomectomy
11/21 – Phallus preserving vulvovaginoplasty
11/28 – Vaginal preserving phalloplasty
12/5 – Phalloplasty
12/12 – Metoidioplasty
12/19 – Vulvovaginoplasty
12/26 – Hysterectomy with and without oophorectomy
1/2 – Scrotoplasty
1/9 – Body contouring to add curves or to remove curves
1/23 – Breast augmentation
1/30 – Chest contouring– fully flat or not, retain nipples or not (mastectomy)
2/6 – Implants – pecs, hip, and butt
2/13 – Vocal surgery to raise or lower pitch
2/20 – Facial surgeries
2/27 – Botox
3/6 – Fillers
3/13 – Managing Hair
Download our patient handout of expected time off after work after various gender affirming surgeries.