You may have seen Erin in the Morning’s journalism on the upcoming Trump administration report on gender affirming care. Like the EITM crew, we expect whatever is published will be a gross misrepresentation of the body of scientific evidence to date. It will be biased against gender affirming care. It will be written with the goal of abolishing gender care. It will very selectively choose flawed studies that do not reflect the full impact of the large body of scientific evidence that is available: trans health care is safe, it is medically necessary, regret rates are extremely low, and it should be available to youth and adults. Trans health care saves lives. Restricting and denying it can be deadly.
Content Note: we’ll be discussing an article in this blog that has statistics about trans youth suicidal ideation and behavior.
Preserving information is going to be vital in the coming days. We’re planning on doing our part: as we are able, we will be posting the major studies in trans health and discussing what they actually say about trans health care.
We’ve written previously about the UK’s version of an unscientific report targeting gender care: the Cass Report. We expect to write about and share others’ writings about the impending current administration’s report.
Trans health care and knowledge is NOT NEW SCIENCE. It is NOT EXPERIMENTAL
Formal medical transition as a field of study is over 100 years old. The first affirming surgeries were done in the 1920s. Informal and DIY (do-it-yourself) care is eons older.
While concepts of gender have changed over time, we have centuries of written histories of people who we would now call transgender, and millennia of oral histories. In modern medical science, Dr. Magnus Hirschfeld founded the Institute for Sexual Science in Berlin in the early 20th century. The archives of the institute were destroyed in 1933 by the Nazis. The first dedicated gender clinics in the United States were openly operating in the 1960s (Johns Hopkins, the University of Minnesota, Northwestern, Stanford, the University of Washington, and the University of Michigan). Gender affirming surgeries were quietly taking place in the United States before then. (Roblee)
A history of trans healthcare and existence may be another blog at another time: it is rich, it is long, and it is expansive. Some readings we suggest (a special shout out to The Gender Doula’s Trans book recommendations):
- The Transgender Child, Jules Gill-Peterson
- Before We Were Trans, Kit Heyam
- Others Of My Kind: Transatlantic Transgender Histories, Annette F. Timm, Alex Bakker, Rainier Hernn, et al.
- Black on Both Sides: A Racial History of Trans Identity, C. Riley Snorton
- Short National Geographic article, “How historians are documenting the lives of transgender people” (soft paywall – email registration)
How To Read A Scientific Study
We can’t provide a deep crash course. But, we can share some basic information on how to read scientific studies so that you can evaluate them on your own. Here’s some of the things you’ll want to think about when you’re reading and evaluating a paper.
What Type Of Study Is It?
- Studies can describe something that happened or ask a question about why or how something happened. Sometimes they do both.
- Descriptive – what happened to whom?
- A case report: here’s a narrative about a patient and their experience.
- A case series: here are the experiences of a group of similar patients.
- A qualitative study: research that tries to explain and understand those experiences.
- Analytic or Quantitative- Crunches numbers (why did this happen? Is Approach A better than Approach B?)
- An observational study
- A cohort: what happened to this group of people over time?
- A cross sectional study: what happened to a group of people at a specific time?
- A case-control study: compares groups of people with and without the condition being studied.
- An experimental study – tries an intervention with a group of people to see what will happen.
- Parallel group: different interventions are tried with different known groups. The outcomes of groups can be compared to each other.
- Randomized group: each individual in the study may receive an intervention or a placebo. Who gets what is randomized.
Typical Types of Medical Science Articles
Not every paper published in a journal is a presentation of the results of an experiment.
The general types of papers are:
- Original Article – new scientific information, often “hey, check this out!” May not have statistics, or robust statistics.
- Case Report – as we mentioned above – this is a description of something that happened to a specific person. No comparative statistics, but there may be descriptive information (age, vitals, etc.)
- Technical Note – new technology information, also a “hey, check this out!” paper.
- Review – not new information, but a combine and contrast of the current body of scientific knowledge about a subject, focusing on recent new developments. This is a “what the current state of X looks like” paper.
- Commentary – the author’s thoughts. Kind of like a letter to the editor in a newspaper, but usually in response to a recently published paper.
- Editorial – the editors of a journal commenting on something about their publishing.
- Article about an Experimental Study – here’s what most people expect to find when they think about “a scientific journal article.” This reports the findings of a study.
- This is often what critics claim we don’t have (see the next section for more info!)
- See “Basic structure and types of scientific papers” for detailed info!
- Note that papers will often not publish the actual data used in the study.
What Does “evaluating a paper” Mean?
We – as individuals, as clinicians and scientists, as groups of clinicians and scientists, and as organizational bodies of clincians and scientists come to an agreement over time about how medicine should be practiced. This is generally known as the standard of care, and standards of care which take into account published evidence is evidence-based medicine. One of the steps is everyone is reading the published papers and asking questions about how likely the authors’ conclusions accurately reflect what is going on in people’s bodies and how to treat people. A “stronger” paper stands up to that questioning better.
Gender Affirming Care IS the Standard of Care. Lots of major medical organizations agree on that.
So much of this comes down to the data and statistics. “Statistics” is a whole field of study that aims to mathematically understand large collections of data and how smaller parts of those collections relate to one another.
A Note On “Evidence Strength” and “Evidence Quality”
For medical studies, these are terms often used to describe how much potential “noise” is in the data and how likely the conclusions drawn from the data accurately describe what is actually happening in people’s bodies.
Randomized control group (experimental) studies are considered to be “stronger” than observational and descriptive studies. Randomized control group studies are narrower in scope both in the questions asked and how the data is collected.
A randomized control group study will have very little, if any personal narrative in the data as compared to surveys or self-reported questionnaires from cohort studies.
A review and analysis of a group of studies is a meta-analysis. A meta-analysis of randomized control group studies is considered to be the highest quality of evidence available.
The Evidence Pyramid

Right Wing Talking Point: Research in gender care is often criticized because the bulk of available studies are descriptive, or observational studies. There are very few experimental studies, and the ones that do exist are parallel group studies.
Why are there so few experimental studies in trans health?
- Because doing a study that ignores previous knowledge on the benefits of an intervention can cause harm to the participants randomized to not receive the intervention. That’s UNETHICAL. Randomized controlled experiments are not appropriate when not providing treatment causes harm.
- Randomized control studies can be ethical during treatment development, or when determining dosaging. Many of the tools we use in trans health were first studied in cis populations and drug formulations/dosages: that’s when randomized control studies were done.
- MONEY and CISHETERONORMATIVITY. No major manufacturer is developing drugs specifically for trans people. There aren’t a lot of us and drug development costs a lot of money. Especially now when research dollars are being slashed and pulled for even including the term “gender.”
- There aren’t many systematic reviews and meta-analyses of trans health care. Much of how we practice medicine is based on studies and learnings about medicine in cis people, and we’ve applied it to trans people. We do have case reports and case series and case-controlled studies and cohort studies, and a lot of clinical expertise and community knowledge.
- Once again: AUTONOMY. We all have the right to decide what we’re going to do with our bodies. An attack on trans care is an attack on autonomy.
We might also see talking points that the harms of not providing gender affirming care aren’t all that bad, anyway. This is also UNETHICAL.
The Sections and Numbers of A Medical Science Article
The articles that we’re reading are typically structured as:
Title: This describes the central question of the study.
Authors: Who were the researchers on this study?
The first page may also include who reviewed or edited the article, and the dates it was submitted, reviewed, accepted, and published by the hosting journal.
Abstract – a short description of the research study, including the methods used, a description of the participants, the results (usually this is a high-level summary of the statistics) and conclusions, where the study authors interpret the results.
These sections are expanded in the body of the paper, where graphs and tables of the study data are presented and discussed.
Introduction – background about the questions that led to the study and what the researchers are trying to find out.
Materials & Methods – the nuts and bolts of the study.
Results – the data!. Charts and graphs!
Discussion – interpretations of the results.
The article will often end with a “what’s next” section, where the authors pose questions for how this research can be continued, a statement of author contributions (who did what) and what funding was available or used.
The final large section of a scholarly article is the references or citations. Here, the authors include the previous studies and sources that informed their work or that they consulted or mentioned in their process.
At the very, very end of the article, you will often see a conflict of interest statement (IMPORTANT for detecting bias!) a publisher’s note and a copyright statement.
Numbers and Statistics You Might See And What They Mean
n – this is the number of participants. Usually people, sometimes other studies or groups of other things. Generally, the higher the n, the more precise the math that interprets how likely the study conclusions can be. Conclusions drawn from a study of 20 people might not be as likely to apply to the larger general population when compared to conclusions drawn from a study of 2,000 people. A single study may have many
P-value – this is the statistical significance. The smaller the p, the more likely that the study found information that didn’t happen by chance. A p value less than 0.05 is the generally accepted benchmark for “yes, what this study found is likely to be a cause/effect relationship.”
Alpha Coefficient (𝜶)- when a measurement has multiple parts (such as a questionnaire) the alpha coefficient weighs how each individual item within the measurement is consistent across the whole. In the questionnaire, it would measure how the answer to one of the questions can predict the answer to every other question. An alpha coefficient closer to 1 indicates that the items within the measurement are more reliable. An alpha coefficient that is a negative number indicates that the items incorrectly predict the answers to the other questions. An alpha coefficient of 0 indicates that there is no predictive value.
CI – Confidence Interval – this is the likelihood that the study, if repeated 100 times, would find the same results. The commonly accepted benchmark for a valid study is a CI of 95%. A higher CI means that the results are more reliable.
OR – Odds Ratio – this is a measure of the strength of the connection between two events. A higher odds ratio means that true cause and effect is more likely. The actual measure ment is the likelihood that effect B will happen in response to event A, compared to effect B happening without event A happening first.
Clinical Significance – different from statistical significance.Findings that are not statistically significant (see p-value above) may still help clinicians make care decisions and recommendations. This is especially important in studies with small sample sizes (the n) where there aren’t enough data points to generate statistically significant results.
Prevalence – the number of a specific event within a population during a certain time period.
Incidence – the number of new cases of an event within a population during a certain time period. Incidence counts new events. Prevalence counts the total number regardless of when the event occurred.
M – Mean – the average of a set of data. The mean of the set (15, 20, 30, 33, 37, 45, 52, 60) is 36.5.
Median – is the middle value in a set of data. If the actual middle value isn’t present, use the average of the two central numbers.. The median of the set (15, 20, 30, 33, 37, 45, 52, 60) is 35 (the average of 33 and 37).
Range – the distance between the lowest and highest values in a set. For the set (15, 20, 30, 33, 37, 45, 52, 60), the range is 60 – 15 = 45.
SD – Standard Deviation – a measurement of how close the values in a set of data are to each other. A lower SD shows that the values are closer together, such as a set of numbers like (1, 2, 3, 4, 5). A higher SD shows that the values are farther apart, such as a set of numbers like (10, 20, 30, 40, 50).
Shall We Give It A Go?
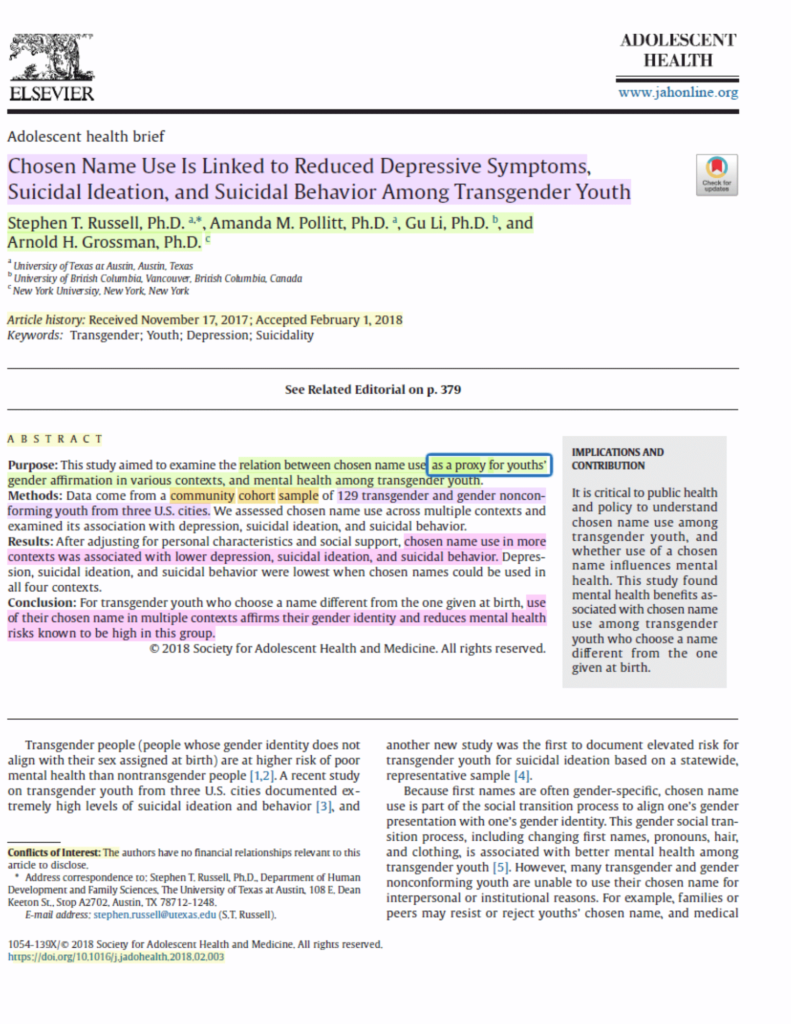
Study: Chosen Name Use Is Linked to Reduced Depressive Symptoms, Suicidal Ideation, and Suicidal Behavior Among Transgender Youth.
Published in the Journal of Adolescent Health, 2018.
On the first page, from top to bottom:
Lavender: the Title. The authors believe that this study indicates that using a transgender youth’s chosen name lowers depressive symptoms, suicidal ideation, and suicidal behavior.
Green: the Authors.
Yellow: the dates that the Journal of Adolescent Health received and accepted the article.
Yellow: First Section of the paper, the Abstract.
Within the Abstract:
Green: the question the study attempted to answer: what is the relationship between using a transgender youth’s chosen name and their mental health? Does it matter what context the chosen name is used in?
Orange: what type of study is this? This is a cohort study: what happened to this group of people over time. Participants in this study were given questionnaires to fill out.
Lavender: the n: 129 youth participated in this study
Pink:
Results: the data showed that use of a chosen name is associated with lower depression, suicidal ideation, and suicidal behavior.
Conclusion: using a chosen name is affirming and reduces mental health risks (an interpretation of the results)
Yellow at the bottom:
Conflicts of interest: the authors did not get paid in ways that might bias the results of this study.
DOI link: this url is where you find the article online.
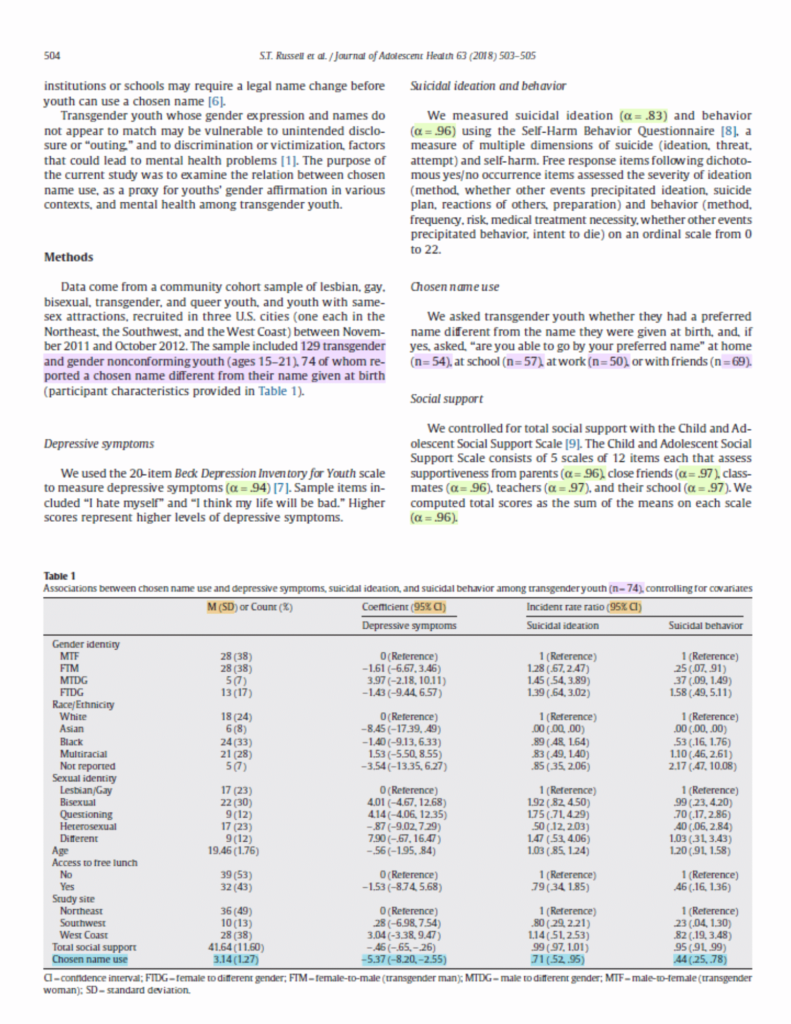
On The Second Page, Top To Bottom:
Lavender, in Methods: the n values
Total number of participants is 129.
74 of those used a chosen name.
Of those that used a chosen name
- 54 used at home
- 57 used at school
- 50 at work
- 69 with friends
Light Green, Alpha Levels
𝜶 = .94 for Beck Depression Inventory for Youth. An Alpha Level of .94 means that each question in the Beck Depression Inventory for Youth is reliable and can accurately precict the values of the other questions.
Orange, in the Table
M(SD) or Count % – the first number in each row is the mean number of participants who answered Yes to that question. The number in parentheses indicates the range of answers or the percent of answers that were that answer. For Gender Identity, 28 individuals out of 74 using chosen names indicated that they were transfeminine. Of those 74 individuals, 38% chose “MTF” as their Gender Identity.
Coefficient (95% CI)– For Depressive Symptoms, the first number describes how each group compared to the reference group. The number in parenthesis shows the expected range of values if there were 100 answers.
Incident rate.
Ratio (95% CI) – for Suicidal Ideation and Suicidal behavior, the number in each row is the count of these events. The number in parenthesis would be the expected count range if there were 100.
Blue, in the Table
Chosen name use – 3.14 (1.27) the mean number of contexts (home, school, work, friends) in which youth were able to use their chosen names was 3.14. The standard deviation for the number of places where chosen names could be used was 1.27. So, the average youth in the study was able to use their chosen name in about 3 out of 4 contexts. Most youth were able to use their chosen names between 2 and 4 places (3.14 minus 1.27 and plus 1.27).
Depressive symptoms
The use of a chosen name in just one context lowered the rate of depressive symptoms by 5.37 points in the measurement scale. If run 100 times, the greatest reduction expected would be 8.2 points and the lowest reduction expected would be 2.55 points.
Suicidal Ideation
Among youth who could use their chosen name, fewer had suicidal ideation compared to the reference group (.71 compared to 1.0) This is a decrease in suicidal ideation of 29% (100 minus 71) The expected range for this reduction was 0.52 to 0.95 (a decrease of 5% to 48%).
Suicidal behavior
Among youth who could use their chosen name, fewer had suicidal behaviors compared to the reference (0.44 versus 1.0) – a decrease of 56%. The expected range for this reduction was 0.25 to 0.78, a decrease of 22% to 75%.
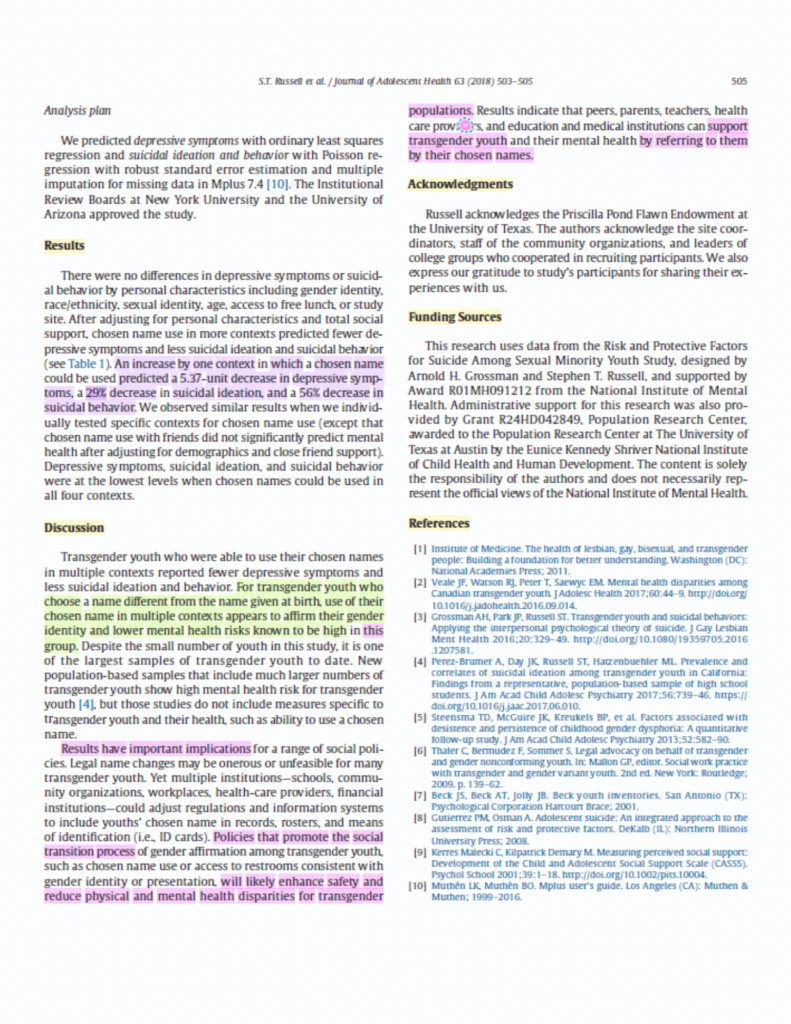
Page Three
Yellow – Labeled sections of the paper
Lavender – the study results: An increase by one context in which a chosen name could be used predicted a 5.37-unit decrease in depressive symptoms, a 29% decrease in suicidal ideation, and a 56% decrease in suicidal behavior. (you can also see this on the bottom row of the table on page 2!)
Light Green – What the authors think this study means (rather than what the data says).
Pink – how the results of this study can be used to improve mental health in transgender youth.
It can be helpful in the Discussion section to go back to the question the authors told us they were asking in the Abstract: what is the relationship between using a transgender youth’s chosen name and their mental health?
You did it!
It can often be helpful to read a scientific paper multiple times. You’re not expected to understand it on the first read. It can be so much easier if you approach it in pieces.
- Read the title, abstract, and the introduction, then all of the headings, then the conclusions.
- Read the whole thing.
- Go back and pore over the tables and data.
- Read it all over again. If reading a scientific article for professional reasons, this pass is where you would heavily inspect the paper for methodology, potential bias, weaknesses, and implications for your own work.
For in-depth information on how to read a paper, see How to Read a Paper (via Stanford.edu). The above points were paraphrased from this resource.
We intend to share several studies over the next few weeks or months, with a similar discussion of the guts of the papers, so stay tuned for more discussion of what the studies about transgender medicine actually say.
References and Resources
Roblee, C., Keyes, O., Lane, M. and Kuzon, W. (2024) “A History of Gender-Affirming Surgery at the University of Michigan: Lessons for Today”. Seminars in Plastic Surgery.
Abdullah Al Noman, Onusree Sarkar, Tanzia Mohsin Mita, Khadiza Siddika, Fahmida Afrose,
Simplifying the concept of level of evidence in lay language for all aspects of learners: In brief review, Intelligent Pharmacy, Volume 2, Issue 2, 2024, Pages 270-273, ISSN 2949-866X, https://doi.org/10.1016/j.ipha.2023.11.002. (https://www.sciencedirect.com/science/article/pii/S2949866X23001168)
Shreffler J, Huecker MR. Hypothesis Testing, P Values, Confidence Intervals, and Significance. [Updated 2023 Mar 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557421/
Szumilas M. Explaining odds ratios. J Can Acad Child Adolesc Psychiatry. 2010 Aug;19(3):227-9. Erratum in: J Can Acad Child Adolesc Psychiatry. 2015 Winter;24(1):58. PMID: 20842279; PMCID: PMC2938757.
Peh WC, Ng KH. Basic structure and types of scientific papers. Singapore Med J. 2008 Jul;49(7):522-5. PMID: 18695858. https://pubmed.ncbi.nlm.nih.gov/18695858/
Deaton A, Cartwright N. Understanding and misunderstanding randomized controlled trials. Soc Sci Med. 2018 Aug;210:2-21. doi: 10.1016/j.socscimed.2017.12.005. Epub 2017 Dec 25. PMID: 29331519; PMCID: PMC6019115.
Tenny S, Brannan JM, Brannan GD. Qualitative Study. [Updated 2022 Sep 18]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470395/
https://www.sciencedirect.com/topics/computer-science/coefficient-alpha
Centre for Evidence-Based Medicine, Study designs: https://www.cebm.ox.ac.uk/resources/ebm-tools/study-designs
https://www.nimh.nih.gov/health/statistics/what-is-prevalence