Menstrual suppression is a very common health goal, and not just for trans folx.
Content Note: We’ll be discussing menstruation (periods, bleeding,) and may use medical and anatomical terms.
The Whys of Menstrual Suppression
There are many reasons why a person might not want to have a period. Some very common reasons are:
- Euphoria!
- Freedom from tracking, preparing for, or experiencing menstruation.
- Being in a body that works more like yours.
- Bodily autonomy.
- Other: _________________________________ (what’s yours?)
- Dysphoria relief!
- from having a monthly cycle or the experience of the hormone cycles which create menstruation.
- from the physical sensations of menstruation.
- from the visual experiences of menstruation.
- Other: _________________________________
- Convenience!
- Manage intense/rough/bad PMS or periods and premenstrual dysphoric disorder (PMDD).
- Manage endometriosis.
- Manage migraines triggered by hormonal fluctuations.
- Manage bleeding disorders.
- Support individuals with limited mobility or dexterity.
- Other: ______________________________________
- And…because you want to.
How Can We Achieve Menstrual Suppression?
Temporary Methods:
These medicines range from very inexpensive to very expensive and some must be taken every day. Others may be used every few days, weekly, every few weeks, monthly, and some may last for years.
Some things to think about and discuss with your medical provider:
- Do I want the changes that occur with taking androgens like testosterone?
- Is a method containing estrogen or that could have estrogenic effects ok?
- Estrogens may cause dysphoria.
- Synthetic estrogens may raise the risk of stroke or blood clots.
- How disruptive would it be if I had spotting or breakthrough bleeding?
- How often do I want to be taking/using my chosen method?
- Is insurance an option? What is my budget?
- Do I want to avoid anything that requires a pelvic exam, a procedure done by someone else/in a medical office, or touching my genitals?
- Do I want to use something that is easily hidden?
- Do I want or need contraception?
- Do I experience pelvic pain or have endometriosis? (Some methods are also used to treat endometriosis.)
These kinds of medications often work by preventing the build-up of endometrial lining in the uterus. It is this lining that is shed and leaves the body during menstruation. The medical term for stopped periods is amenorrhea.
TLDR? We created a chart with highlights of the below information, available for download.

Testosterone
Forms available: Injection, gel, pill, nasal spray, implant
Cost: varies, depending on form and insurance
Stopping periods is one of the most frequently desired effects of taking testosterone.
It may take several months for menstruation to completely go away on T. Breakthrough bleeding is uncommon, except when doses are missed or late. Testosterone is a controlled substance, so prescriptions may be more difficult to obtain, and can be expensive. Testosterone will cause many other changes in your body as well, learn more on our All The T page.
GnRH antagonists/agonists – “blockers”
GnRH stands for “gonadotropin-releasing hormone”.
GnRH agonists and antagonists both stop the pituitary gland from making the hormones follicle-stimulating hormone (FSH) and luteinizing hormone (LH.) FSH and LH tell the gonads in the body (ovaries and testicles) to make sex steroid hormones like testosterone, estrogen, and progesterone.
Agonists “ramp up” the effect of a hormone. In the presence of a GnRH agonist, the gonadotropin hormone receptors in the pituitary gland get feel full and think that the body already has enough FSH and LH, so it doesn’t make more. GnRH agonist examples include leuprorelin, triptorelin, and histrelin.
Antagonists take the place of hormones in receptors and “block” them. When a GnRH antagonist is around, gonadotropin receptors in the pituitary gland never get the message to make FSH and LH, so they don’t make any. A GnRH antagonist used in gender medicine is elagolix.
Blockers may cause a surge of hormones or the symptoms they are treating before they calm everything down. Read our Blockers FAQ.
Cost: very expensive; patient assistance programs do exist and insurance may cover. With insurance will almost certainly need prior approval. Blockers can be difficult and frustrating to access.
Blockers are usually VERY effective at stopping periods after the initial surge phase.
Many people get blocker injections in a medical office, but they can be done at home.
Depot leuprolide / leuprolide acetate
Muscular injection, every month or every three months
Triptorellin acetate
Muscular injection, twice a year.
Histrelin implant
Implant, placed in the buttocks.
A small implant is surgically placed once a year in a doctor’s office. Can be done under anesthesia.
Elagolix
Pill, taken by mouth once or twice a day.
Brand name Orilissa – this works by lowering the amount of estrogen in the body. Like other blockers, it can be very expensive. Do not take elagolix with contraceptive methods containing estrogen.
Danazol
Capsule by mouth, twice a day.
Cost: less than $3/day (generic cash price, per GoodRx.)
Danazol is an inhibitor rather than a blocker – it slows down the pituitary gland and is anti-estrogenic. It has some androgenic effects, and can cause changes in the body similar to taking testosterone, such as facial hair growth, deepening of the voice, and acne, but these effects aren’t as strong as taking testosterone. Can be expensive.
A study looking at cis and transgender individuals using danazol, a daily dose of 400mg achieved suppression of menstruation in 85% of the trans participants and 79% of the cis participants. (Scatoni)
SERMs
SERMs are selective estrogen receptor modulators. They work by stopping estrogen molecules from binding to receptors in tissues in the body. Some SERMs target specific kinds of estrogen-sensitive cells like breast or uterine cells. Read up on SERMs here.
Raloxifene
Pill, taken once a day by mouth.
Cost: less than $0.50/day (generic cash price, per GoodRx)
Anastrazole
Pill, taken once a day by mouth.
Cost: less than $0.50/day (generic cash price, per GoodRx)
Synthetic Progestins
Synthetic progestins are human-made chemicals similar to progesterone made by the body.
Some progestins are also prescribed as contraception. Contraception is currently covered by ACA insurance plans.
Drospirenone
Pill taken once a day by mouth.
Cost: $7.15/day (generic cash price, per GoodRx)
Has anti-androgenic effects, so may not be a good match for people who may also be interested in testosterone now or later.
Norethindrone acetate (NETA)
Pill, taken once a day by mouth.
Cost: less than $0.50/day (generic cash, per GoodRx)
When used to stop menstruation, it is a pill taken by mouth every day at about the same time. Missed or late dosages may cause bleeding to happen. A small amount of NETA may convert to estrogen in the body.
Norethindrone (NET) “the mini pill”
Pill, taken once a day by mouth.
Cost: less than $0.50/day (generic cash, per GoodRx)
A progestin-only oral tablet taken daily. Inexpensive, but may be less effective, and for highest effectiveness, needs to be taken at the same time every day.
Depot medroxyprogesterone (DMPA) “Depot-Provera”
Injection every 11- 15 weeks
Cost: less than $0.50/day (generic cash, per GoodRx)
May be used as contraception.
DMPA is a common progestin-only contraceptive that is given by injection every 11 – 15 weeks.
It is very effective at stopping menstruation: 50% – 60% of users had stopped periods at one year and 70% at 2 years. It can also be used to treat endometriosis. May decrease bone density. Widely available and can be inexpensive or free when covered by insurance, but injections may need to be done in a medical office.
Oral medroxyprogesterone acetate (MPA)
Pill, taken once a day by mouth.
Cost: less than $0.50/day (generic cash, per GoodRx)
Progestin IUDs (intra-uterine device)
Brand names: Mirena, Liletta, Kyleena, Skyla
Hormonal IUDs are small medical devices that are placed within the uterus.
Cost varies.
May be used as contraception.
Hormonal IUDs (may be called IUS) slowly release small amounts of progestins into the uterus, and are approved for 3 to 8 years of use. Requires a pelvic exam and insertion and removal in a doctor’s office, which may be painful or trigger dysphoria. Can be expensive, but should be covered under an ACA plan as contraception. Some users experience pelvic pain.
In a study of cis users, 50% had stopped periods at 1 year, and 60% at 5 years. Spotting may occur, and flow is often greatly reduced in amount and duration if periods are not stopped.
Combined hormonal contraceptives
These methods contain both estrogen and progestins, so may not be a good match for people who wish to avoid estrogen. Cost varies, but contraceptives are currently covered by ACA insurance plans.
Oral Contraceptives “the pill,” “birth control”
Pill taken once a day by mouth.
Cost: varies depending on formulation.
Pills are typically taken once a day and may be time sensitive. For menstrual suppression, they are taken continuously. Some users may find packaging dysphoric. Periods are stopped for 70% of users at 1 year.
Patches
Patch placed on the skin for a week, then replaced.
Cost: varies, usually less than $2/day (generic cash, per GoodRx)
For contraception, patches are worn for three weeks, then a break of one week is taken. For menstrual suppression, patches are used continuously. May cause skin irritation in some people.
Vaginal Rings
Soft, flexible plastic rings that are placed in the vagina and replaced every three weeks.
Cost: varies, usually less than $2/day (generic cash, per GoodRx)
For menstrual suppression, rings are used continuously. Inserting and removing the ring may cause dysphoria for some people.
Permanent Methods
Hysterectomy – the removal of the uterus, with or without the cervix. Can be hard to get and expensive. May also require significant recovery time where activities are limited. Hysterectomy may be covered by insurance.
Uterine ablation – may be semi-permanent. Uterine ablation is a surgical procedure that destroys the uterine lining. It may stop periods completely, or make them much lighter. Ablation may be covered by insurance.
Studies on effectiveness of menstrual suppression methods in TRANS PEOPLE!
Every body is different, and each method may work on a different time scale. Many people will experience spotting or breakthrough bleeding until their chosen method fully kicks in.
In Adolescents:
In a study of 220 transgender people under age 24 using a variety of methods, less than half had their periods stop within 6 months. Most of the participants used one method. Individuals using more than one method often added a second one when the first one did not fully stop menstruation.
Testosterone alone: 151 days, about 5 months.
Norethindrone acetate: 78 days, about 2.5 months
Depot leuprolide: 77 days, about 2.5 months
T plus norethindrone acetate: 188 days, a little over six months
T plus depot medroxyprogesterone: 168 days, about 5.5 months.
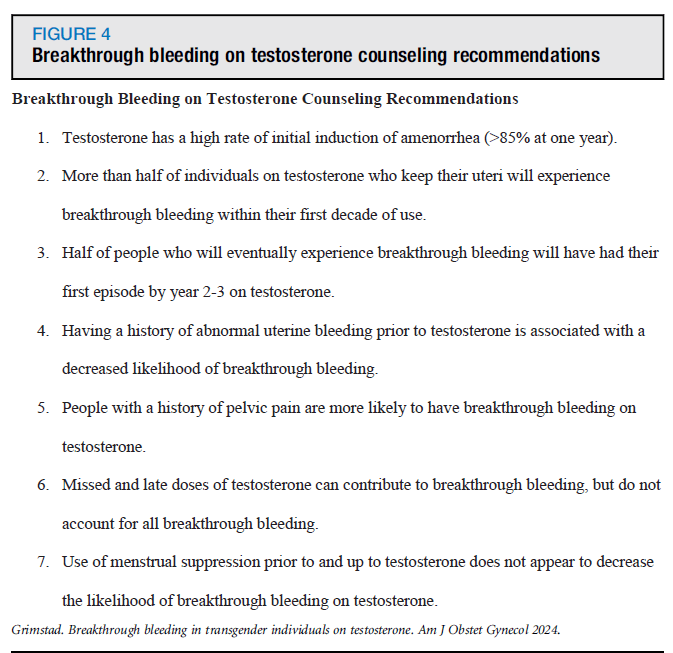
Studies on adults using testosterone:
- 85% stopped menstruating by the end of the first year of T.
- Many people have this happen within 3 – 6 months (Roden)
- 33% experienced breakthrough bleeding after the first year.
- Missing doses or taking lower doses than usual appear to be a trigger for breakthrough bleeding
Older adolescents and adults (17+) using danazol: (Scatoni)
- Time to suppression in a study of 46 individuals was between 1 and 4 months.
AT QUEERDOC
We know that stopping menstruation can be a super cool and highly desired effect of gender affirming care, and if a patient is able to menstruate, we want to know how they feel about it!
We typically use testosterone, depo-provera, or raloxifene most often to stop periods.
Where Did We Find All Of This Information?
Clinical experience and community knowledge, and we’re so thrilled to see more and more studies about transgender medicine being done and written about, including many of the below:
https://www.webmd.com/drugs/2/drug-6024/norethindrone-acetate-oral/details
https://medlineplus.gov/druginfo/meds/a604034.html
https://www.mayoclinic.org/tests-procedures/depo-provera/about/pac-20392204
V.I. Alaniz, J.L. Sheeder, G.T. Whitmore, M.D. Wilde, K.J. Hutchens, N.J. Nokoff, D.H. Reirden, P.S. Huguelet, Menstrual Suppression in Adolescent and Young Adult Transgender Males, Journal of Pediatric and Adolescent Gynecology, Volume 36, Issue 2, 2023, Pages 116-121,
ISSN 1083-3188, https://doi.org/10.1016/j.jpag.2022.10.007. (https://www.sciencedirect.com/science/article/pii/S1083318822003047)
Frances W. Grimstad, Elizabeth R. Boskey, Rachael S. Clark, Cecile A. Ferrando,
Incidence of breakthrough bleeding in transgender and gender-diverse individuals on long-term testosterone, American Journal of Obstetrics and Gynecology, Volume 230, Issue 4, 2024, Pages 434.e1-434.e10, ISSN 0002-9378, https://doi.org/10.1016/j.ajog.2023.12.036.
(https://www.sciencedirect.com/science/article/pii/S0002937824000024)
Frances W. Grimstad, Elizabeth R. Boskey, Rachael S. Clark, Cecile A. Ferrando,
Management of breakthrough bleeding in transgender and gender diverse individuals on testosterone, American Journal of Obstetrics and Gynecology, Volume 231, Issue 5, 2024,
Pages 534.e1-534.e11, ISSN 0002-9378, https://doi.org/10.1016/j.ajog.2024.06.004.
(https://www.sciencedirect.com/science/article/pii/S0002937824006677)
Roden RC. Reversible interventions for menstrual management in adolescents and young adults with gender incongruence. Therapeutic Advances in Reproductive Health. 2023;17. doi:10.1177/26334941231158251
Scatoni A, Roberts Z, Boskey ER, et al. Danazol’s use for menstrual suppression in transgender individuals: A retrospective multi-site cohort study. Women’s Health. 2024;20. doi:10.1177/17455057241265081
Hillard PA. Menstrual suppression: current perspectives. Int J Womens Health. 2014 Jun 23;6:631-7. doi: 10.2147/IJWH.S46680. PMID: 25018654; PMCID: PMC4075955.
Defreyne J, Vanwonterghem Y, Collet S, Iwamoto SJ, Wiepjes CM, Fisher AD, Schreiner T, Heijer MD, T’Sjoen G. Vaginal bleeding and spotting in transgender men after initiation of testosterone therapy: A prospective cohort study (ENIGI). Int J Transgend Health. 2020 Feb 12;21(2):163-175. doi: 10.1080/26895269.2020.1719951. PMID: 32935087; PMCID: PMC7489282.
Stay Checked-In With QueerDoc!
(an email every month or so)