From now until sometime in Spring 2023, we’ll be writing about gender affirming surgeries and procedures. We’re starting with bottom surgeries and will end with office visit procedures such as fillers and botox. This week, we’re discussing phalloplasty. You may see the term shortened to “phallo.”
Content advisory: we will be using anatomical terms and discussing surgical procedures in this article and this series. External sites that we link to may contain graphic images.
What is phalloplasty?
Phalloplasty is the creation of a penis. This surgery was originally developed to treat cis men who had experienced cancer or tissue trauma, and is still used in those circumstances.
Phalloplasty is a complex process, and usually involves multiple surgery stages with time for healing in between each stage. There are also several different techniques for phalloplasty. We’ll discuss some of the more well-known ones. Phallo.net is an excellent resource for additional in-depth information.
The simplest explanation of phalloplasty is that a section of skin and underlying tissues from one part of the body (the donor flap) is used to create the shaft of the new penis. The shaft is then attached to the groin and blood vessels and nerve fibers are connected to existing structures. There can be any number of associated procedures which we will explain below:
- urethral lengthening (allows you to pee out of the tip of your penis)
- glansplasty (additional visual changes to the head of the penis)
- scrotoplasty (creates a scrotum)
- clitoroplasty (changes the structure of the clitoris)
- vaginectomy (removal of the vagina) and hysterectomy (removal of the uterus)
- oophorectomy and salpingotomy (removal of the ovaries and fallopian tubes)
- monsplasty (sculpting of the fat pad on the front of the groin below the belly)
- penile implants (to have erections)
- testicular implants (to add balls to the scrotum)
- secondary skin grafts (may be needed to help heal the main skin graft area)

Urethral lengthening increases the complexity of surgery and possible risks, but will allow you to pee out of the tip of the penis and make peeing while standing easier. Some surgeons will require vaginectomy (removal of the vagina and closure of the vaginal opening) and hysterectomy (removal of the uterus, the fallopian tubes, and the cervix,) if urethral lengthening is desired. There is evidence that vaginectomy reduces the complication rates of urethral lengthening and can provide tissue to create the new urethra.
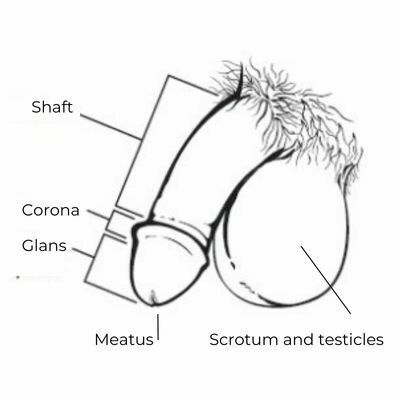
Glansplasty is the creation of a head to the penis. If urethral lengthening is also chosen, a meatus–the opening at the end of the urethra where urine leaves the body–is created as well. Glansplasty can be used to enhance aesthetic details of the penis, such as a corona ridge to look more like a circumcised penis, and medical tattooing can update tissue color and provide visual details.
Scrotoplasty is the creation of a scrotum at the base of the penis. Labial tissue is often used to create the scrotum, but donor tissue from another part of the body may be used, as well. If urethral lengthening is not desired, the urethra will be behind the scrotum, towards the back of the body.
Clitoroplasty: the clitoris may be buried in the base of the new penis. It may also be left as is.
The individual can choose to have a vaginectomy (removal of the vaginal canal and closure of the opening) or can choose to keep the vagina intact (read our blog on vaginal-preserving phalloplasty!) If vaginectomy is chosen, a hysterectomy (removal of the uterus) will be required. The individual can choose to have one or both ovaries and the fallopian tubes removed at the time of hysterectomy.
Monsplasty shapes the tissue underneath where the penis will be placed (the mons pubis) for a flatter appearance and transition from the belly to the groin. Some surgeons use fat removed during this process to fill out the scrotum, instead of implants.

Penile implants are devices placed inside the penis that allow for erections. Some are rods, which may be bendable or unbendable (always erect.) Some are inflatable cylinders that uses a pump and salt water to fill the cylinders and cause an erection. When not erect, the salt water stays in a surgically implanted reservoir in either the abdomen or scrotum. The pump is generally in the scrotum. Phallo.net has a good write-up about how penile implants work.
Testicular implants are egg-shaped saline pouches that are filled with salt water or all-silicone eggs. They are implanted in the scrotum and provide the look, weight, and feel of testicles. Some surgeons use fat moved from another part of the body to create bulk in the scrotum.
Secondary skin grafts may be used to help heal the donor flap site. A smaller piece of skin is removed from another part of the body and connected to the donor site. The original donor site may be covered with a special film to help prevent infection and increase healing before the secondary skin graft or instead of a skin graft. In a graft, the edges are connected to the new site, but blood vessels are not. A flap will have either an existing blood vessel maintained or microsurgery done to connect blood vessels at the new site.
OHSU has an excellent guide to phalloplasty. It doesn’t discuss all the options for phalloplasty, but does provide an overview of the process from start to finish. OHSU also has developed a new treatment program to help maintain sexual sensations with the input of people with lived experience.
There are two types of donor flaps:
- the pedicled flap – this is an older technique, where a section of skin and the underlying tissues is lifted up and rotated, then formed into a tube and reattached to the groin. Pedicle flaps retain the connection to an original nerve or blood vessel and do not require microsurgery. They may be easier to heal and less expensive.
- the free flap – this is a newer technique. In a free flap phallo, a section of skin with underlying tissues is completely separated from another part of the body, formed into a tube, and reattached at the groin. Microsurgery to connect blood vessels and nerves is required, so a free flap procedure may take longer in the operating room and to heal, and may be more expensive.
Types of phalloplasty, in order of complexity and risk:
- simple tube – when no urethra lengthening is desired
- tube-within-a-tube – when urethra lengthening is desired
- hybrid – when neither option is suitable for the patient
Phalloplasty Tissue Graft Donor Sites
The choice of “flap” site can affect the final appearance, length, girth, and sensation of the new penis. Opting for urethral lengthening may limit where the donor graft comes from, as well. Your body type – your natural fat layer under your skin and how you scar may also affect your choice of donor site.
Skin sensation and erotic sensation can be obtained, but depend on a few factors:
- the level of skin sensation felt in the original skin
- what kind of nerves are in the tissue being moved
- sensory nerves will continue to be able to transmit touch signals
- motor nerves will not transmit touch signals (these types of nerves tell muscles to move)
- if the nerves are being re-routed and connected to other nerves or left in place

The most common types of phalloplasty are:
- radial arm free flap: uses forearm skin from the non-dominant arm
- can be used with urethral lengthening
- skin starts out sensitive and nerves can be re-routed
- less girth is obtainable
- less length is obtainable
- will have a visible forearm scar and may need a second skin graft to help the arm heal
- may limit hand and wrist mobility and cause chronic pain
- significant time and energy spent on occupational and physical therapy is important to reduce these outcomes
- anterior lateral thigh flap: uses skin from the thigh
- can be free-flap or pedicled
- can be used with urethral lengthening
- the skin is less sensitive than forearm skin
- free-flap can re-route nerves
- pedicled does not re-route nerves and will have less erogenous sensation
- more girth is obtainable
- more length is obtainable
- may have less-obvious or easier to cover scars
- a second skin graft may be needed for the donor site
- may limit leg strength and cause chronic pain
- abdominal flap: uses skin from the abdomen
- generally pedicle flap
- cannot be used with urethral lengthening
- the skin is less sensitive than forearm skin, and nerves will not be re-routed
- medium girth
- less length is obtainable
- less scarring or easier to cover scars compared to other techniques
- a second skin graft is likely not needed
- may experience chronic nerve pain
- dorsal free flap: uses muscle and skin from the side and back
- can be used with urethral lengthening
- little skin sensation
- the nerves in the flap don’t transmit sensory messages (they’re motor nerves)
- more girth is obtainable
- more length is obtainable
- scarring is along the torso, and may not require a second skin graft
- may limit the mobility of the torso and arm and cause chronic pain
- also known as “MLD”
- fibula flap: uses tissue and bone from the lower leg
- can be used with urethral lengthening
- skin sensation is not expected but may occur
- however, the existing nerves can be re-routed to a clitoral nerve
- more girth is obtainable
- more length is obtainable
- fibula bone is grafted to the pubic bone and provides shaft rigidity instead of an erectile implant
- scarring is on the lower leg
- may limit strength and balance on the donor leg and cause chronic pain

When: Expected Prep and Recovery for Phalloplasty
Prep and recovery will be affected by the type of phalloplasty chosen, the donor location, additional procedures desired, and the overall health of the individual.
We discuss general prep for bottom surgeries in an earlier blog – getting ready for your recovery time can make a huge impact on your healing. Also check out our pre-surgery checklist. As phalloplasties are often done in several separate surgeries or stages, you may have to prep and go through your checklist several times. OHSU has an INCREDIBLE phalloplasty resource – you can download it here.
Hair removal on the donor site may take several months to a year to complete. Some surgeons prefer that if a hysterectomy is desired, it is done at least three months prior to phalloplasty.
If additional procedures such as hysterectomy, scrotoplasty, glansplasty, and implantation of an erectile device are desired, the individual may have several surgical dates, each separated by healing time.
A typical “3-stage” approach for a radial forearm free flap phalloplasty with urethral lengthening, scrotoplasty, hysterectomy, vaginectomy, and penile implants performed by Johns Hopkins:
- Stage 1 – create the penis from the forearm skin graft
- hospital stay of four to five days
- time off from work may be up to 8 weeks
- five to six months for healing
- regular visits with occupational therapy for 6-8 weeks is not uncommon
- Stage 2 – connects old urethra to new urethra, vaginectomy, scrotoplasty, glansplasty
- hospital stay of up to a couple of days
- time off from work may be up to four weeks
- up to a year for healing
- Stage 3 – testicle implants and erectile device implants
- overnight hospital stay
- time off from work may be up to eight weeks
“Single-stage” phalloplasty combines stages 1 and 2. Phallo.net has a great diagram and description of staging options.
How: Common Surgeon and Insurance Requirements
Like other lower surgeries, you will likely need two letters from two different mental health providers for your surgeon, along with a letter from your surgeon and/or hormone provider for insurance. They may require hormone use for a certain period of time or want documentation for why hormones were not part of your journey, and they may wish to know that you have “lived as” for a certain period of time. Some policies may require that you document your support and housing plans during recovery.
If you are a smoker, you will need to quit smoking at least three months prior to each surgery.
Your surgeon or your referring provider will do a physical exam before surgery to confirm that your health is optimized and you have the best chance for a successful procedure(s).
Why: Some Things To Think About When Choosing Phalloplasty
We’ve said it before: form and function.
You probably already know that you want phalloplasty. You may have already thought about metoidioplasty as an option. If you haven’t, stay tuned for next week’s blog.
Your goals for your genitals can help guide what kind of phalloplasty is best suited for you:
- do you want more or less girth and length?
- do you want to pee standing up from the tip of your penis?
- do you want to be able to use your penis for penetration?
- how much touch sensation do you want on the shaft of your penis?
- how important are visible scars to you?
- how might decreased mobility or weakness in the donor flap area affect you?
- what do you want your penis to look like?
These factors, along with your body type, will inform the discussions you have with surgeons about which method and technique is best for you.
Where: Surgeons Who Offer Phalloplasty
There are many surgeons doing phalloplasties, and more surgeons are learning the techniques. Phallo.net lists surgeons who offer each type of phallo on their information pages and has a directory.
Other tips for finding a surgeon:
We have a limited database of surgeons by procedure on our Gender Affirming Surgery page. It was designed for our internal use, so it contains medical terminology. Use with caution.
Some other directories of surgeons include the following:
- TransHealthCare.org
- findplasticsurgery.org
- WPATH Provider Directory
- OutCare Health
- ftmsurgery.net
- The r/TransSurgeries wiki on Reddit
Dr. Blair Peters at OHSU is pioneering in the field and is queer-identified. You can follow them on Insta at @queersurgeon.
Download our Questions to Ask Your Surgeon Before Bottom Surgery handout.